This, According to the American Heart Association:
Women face a disproportionate burden of stroke mortality and disability. Biologic sex and sociocultural gender both contribute to differences in stroke risk factors, assessment, treatment, and outcomes. There are substantial differences in the strength of association of stroke risk factors, as well as female-specific risk factors. Moreover, there are differences in presentation, response to treatment, and stroke outcomes in women. This review outlines current knowledge of impact of sex and gender on stroke, as well as delineates research gaps and areas for future inquiry.
Stroke Epidemiology
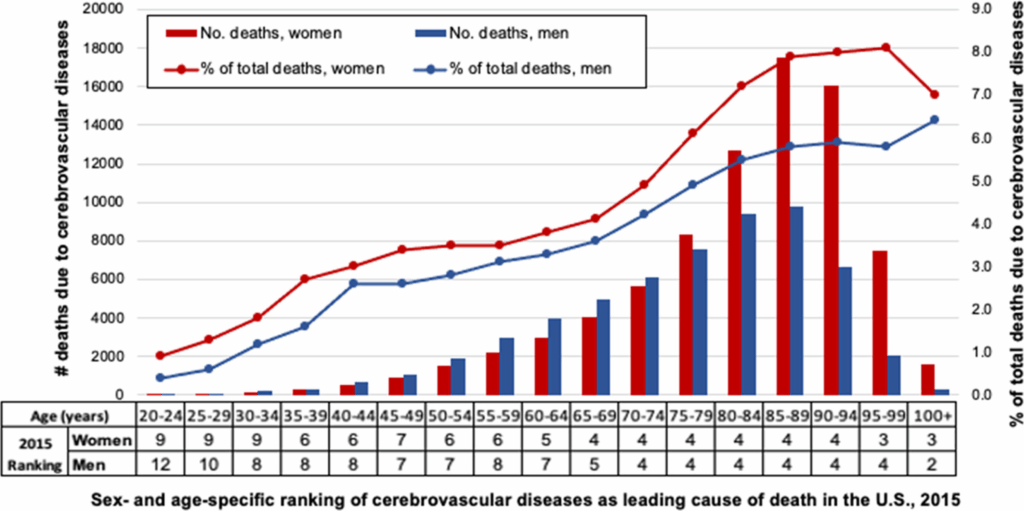
In 2019, the most current year available, stroke was the second leading cause of death worldwide, as well as the second cause of disability-adjusted life-years.1 In the United States in 2019, stroke was the third leading cause of death in women, compared with fifth in men.2 Women accounted for 57.1% of stroke deaths in 2019, with stroke accounting for 6.2% of all female deaths, while comprising 4.4% of all male deaths.2 In total, Approximately 55 000 more fatal strokes occur in women each year than men.3 In the 2015 GCNKSS (Greater Cincinnati Northern Kentucky Stroke Study), stroke case fatality in women exceeded that of men for the first time, even after adjustment for age.4,5 As shown in Figure 1, strokes comprise a greater percentage of deaths in women than men throughout the adult life span (Lichtman et al, unpublished data, 2021).
Globally, the lifetime risk of stroke (from age 25 years onward) is 25.1% in women and 24.7% in men, but there is substantial regional variation.6 There are regional differences with the highest lifetime risks for women in Eastern Europe and East Asia (36.5% and 36.3%, respectively).6 In the United States, the lifetime risk of stroke is higher in women (20%–21%) than in men (14%–17%), for a 55-year-old individual.7 Stroke is more likely to be the first manifestation of cardiovascular disease in women, whereas in men, coronary heart disease is more common.8 The social context for women who experience stroke is important as well. Age at onset of stroke is on average 4 to 6 years older in women than men.4,9 Moreover, women are more likely to be widowed, unmarried, or living alone and have a higher degree of disability in their activities of daily living than men at the time of their stroke.
The following are 6 reasons women have a higher risk of stroke than men, according to Riverside Health:
Stroke risk factors in women include these six reasons:
1. Age – Stroke risk rises as we get older. Statistically, women live longer than men.
2. Atrial fibrillation – This irregular heartbeat, also known as AFib, increases stroke risk among women over age 75 by 20 percent.
3. High blood pressure – High blood pressure is the leading cause of stroke. About one in three women have stage 2 high blood pressure (greater than or equal to 140/90 mmHg), but only half have it under control, according to the Centers for Disease Control and Prevention. High blood pressure strains blood vessels, which can make them rupture.
4. Pregnancy – High blood pressure during pregnancy can cause a stroke.
5. Hormonal medications – For women already at high risk for a stroke, taking birth control pills can increase their risk, especially if they smoke. Hormone replacement therapy in women during menopause slightly increases their stroke risk because it can cause blood clots and increase blood pressure.
6. Migraines – Migraines with aura are associated with ischemic stroke in younger women, especially if they smoke or use birth control pills.
So, what can you do to prevent a stroke?
Here are some stroke prevention tips:
- Eat healthier
- Exercise regularly
- Aim to lower blood pressure and cholesterol
- Quit smoking
- Reach a healthy weight
Sources: American Heart Association, Riverside Health online
1. Vyas MV, Silver FL, Austin PC, Yu AYX, Pequeno P, Fang J, Laupacis A, Kapral MK. Stroke incidence by sex across the lifespan. Stroke. 2021;52:447–451. doi: 10.1161/strokeaha.120.032898
2. Heron M. Deaths: leading causes for 2019. Natl Vital Stat Rep. 2021;70:1–114.
3. Virani SS, Alonso A, Aparicio HJ, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Cheng S, Delling FN, et al; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143:e254–e743. doi: 10.1161/CIR.0000000000000950
4. Madsen TE, Khoury JC, Leppert M, Alwell K, Moomaw CJ, Sucharew H, Woo D, Ferioli S, Martini S, Adeoye O, et al. Temporal trends in stroke incidence over time by sex and age in the GCNKSS. Stroke. 2020;51:1070–1076. doi: 10.1161/strokeaha.120.028910
5. Rehman S, Sahle BW, Chandra RV, Dwyer M, Thrift AG, Callisaya M, Breslin M, Phan HT, Otahal P, Gall S. Sex differences in risk factors for aneurysmal subarachnoid haemorrhage: systematic review and meta-analysis. J Neurol Sci. 2019;406:116446. doi: 10.1016/j.jns.2019.116446
6. Feigin VL, Nguyen G, Cercy K, Johnson CO, Alam T, Parmar PG, Abajobir AA, Abate KH, Abd-Allah F, Abejie AN, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379:2429–2437. doi: 10.1056/NEJMoa1804492
7. Seshadri S, Beiser A, Kelly-Hayes M, Kase CS, Au R, Kannel WB, Wolf PA. The lifetime risk of stroke: estimates from the Framingham Study. Stroke. 2006;37:345–350. doi: 10.1161/01.STR.0000199613.38911.b2
8. Leening MJ, Ferket BS, Steyerberg EW, Kavousi M, Deckers JW, Nieboer D, Heeringa J, Portegies ML, Hofman A, Ikram MA, et al. Sex differences in lifetime risk and first manifestation of cardiovascular disease: prospective population based cohort study. BMJ. 2014;349:g5992. doi: 10.1136/bmj.g5992
9. Petrea RE, Beiser AS, Seshadri S, Kelly-Hayes M, Kase CS, Wolf PA. Gender Differences in Stroke Incidence and Poststroke Disability in the Framingham Heart Study. Stroke. 2009;40:1032–1037. doi: 10.1161/strokeaha.108.542894